Immigration Law
You have a job offer. A U.S. hospital or healthcare facility wants you. Maybe your employer has already mentioned sponsoring you for a green card through Schedule A.
Here's what surprises most internationally trained nurses at this point: the immigration petition is only half the equation. Running alongside it — and just as likely to delay your start date if not handled carefully — is a separate credentialing process that every foreign-educated nurse must complete before they can legally practice in the United States.
A U.S.-trained nurse graduates, passes one exam, and goes to work. A foreign-trained nurse must first prove to U.S. authorities that their education meets American standards, that their clinical English is sufficient for patient care, and that they satisfy a federal screening requirement that has nothing to do with USCIS. None of this is impossible. But none of it is automatic, and the steps are interdependent in ways that catch people off guard.
This article walks through each additional requirement — what it is, why it exists, and what you need to know to get through it efficiently. For a detailed explanation of the employer sponsorship side — the I-140 petition, prevailing wage determination, and Visa Bulletin timeline — see our article on EB-3 nurse sponsorship through Schedule A.

This is the foundational point, and it surprises more nurses than it should.
The United States has no reciprocity agreements with foreign nursing regulatory bodies. A nursing license from the Philippines, Ukraine, India, Nigeria, Romania, or anywhere else carries zero legal authority with a U.S. state board of nursing. It does not grant you the right to practice. It does not shorten the licensure process. It simply confirms that you are a licensed nurse somewhere else.
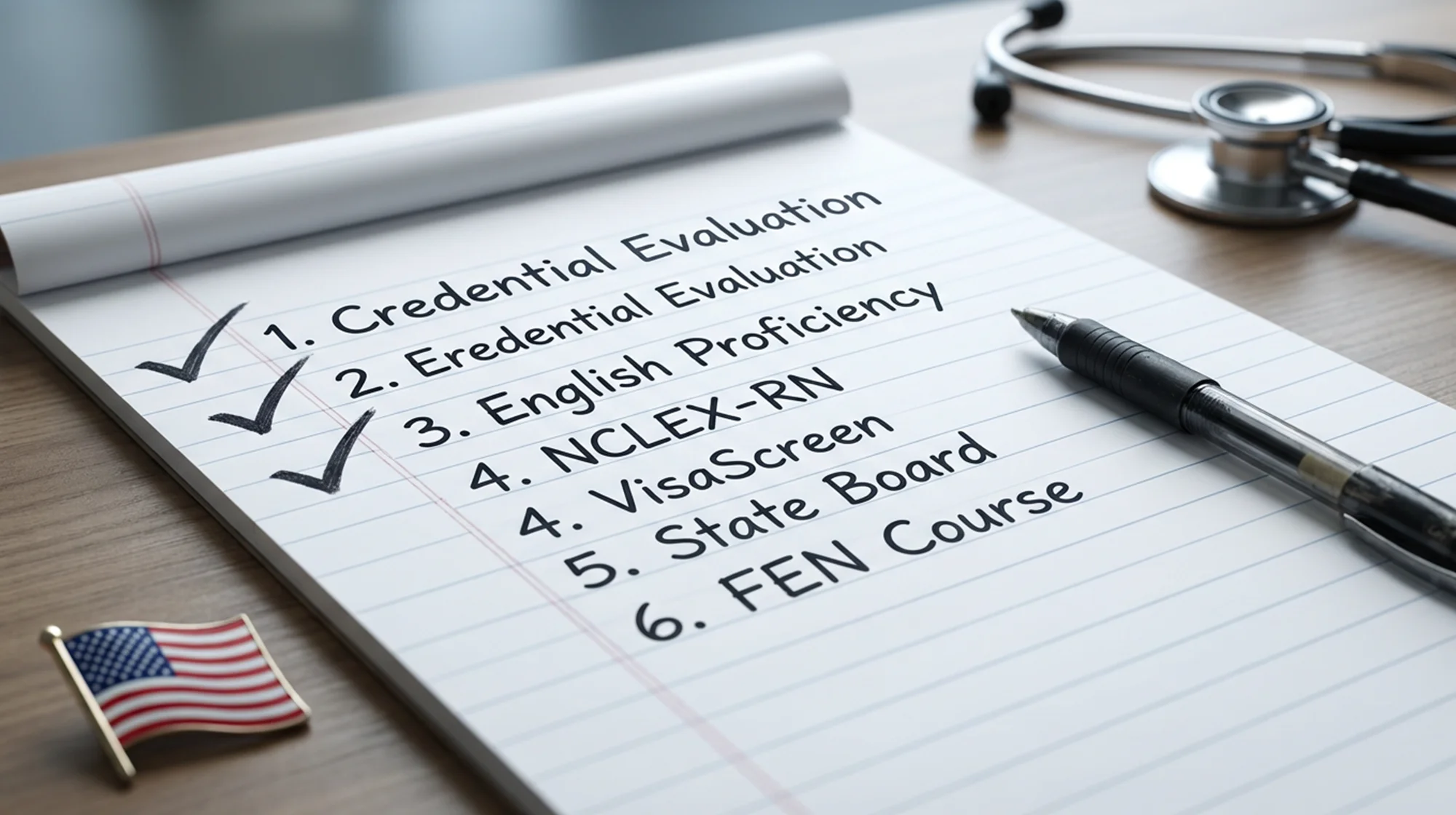
To work as an RN in the United States, you must qualify for a new U.S. license — evaluated from scratch against American standards. That process has several distinct components, each administered by a different agency, each with its own documentation requirements and timeline. Below is what that looks like in practice.
The first thing U.S. state boards of nursing want to know is whether your foreign nursing program covers the same ground as a U.S. nursing degree. They do not take your home country's word for it.
This evaluation is performed through a Credentials Evaluation Service (CES) report, most commonly administered by CGFNS International (now operating as TruMerit). The CES report is not a simple diploma check. It is a course-by-course analysis of your nursing program's theoretical instruction and clinical hours, measured against U.S. curriculum standards.
Evaluators are specifically looking for coverage in five clinical areas: adult medical nursing, adult surgical nursing, pediatric nursing, neonatal nursing, and psychiatric nursing. Many internationally trained nurses have strong preparation in the first three. Psychiatric nursing and gerontology are where programs from many countries fall short — these are not always standard components of general nursing education outside the U.S.
If the evaluation finds that your program lacks sufficient hours in a required area, you will need to complete supplemental coursework at a U.S.-accredited institution before your state board will process your license application. This is not a disqualifier — but it is a delay, and it is one worth knowing about before you start the process.
One procedural point that matters: your official transcripts must be sent directly from your nursing school and secondary institution to CGFNS. Transcripts you carry yourself — even sealed — are not accepted. If your school is in a country where administrative processes move slowly, build time into your plan for this step. It is often the first place timelines slip.
U.S.-trained nurses do not take an English proficiency exam. For foreign-trained nurses, it is almost always required — and the threshold is set deliberately high.
The reason is patient safety. Nurses communicate in high-stakes environments: interpreting physician orders, documenting patient status, responding to emergencies, educating family members on discharge instructions. The speaking requirement in particular reflects the reality that a nurse who reads and writes English competently may still struggle to communicate clearly under pressure in real-time clinical situations.
The major approved examinations are the TOEFL iBT, IELTS Academic, OET (Nursing), and PTE Academic. Each has its own format and scoring structure, and each carries specific minimum score requirements — with the speaking component almost universally held to a stricter standard than the overall score. For example, some state boards require a TOEFL iBT speaking score of 26 while accepting an overall score of 84 or above. The gap between those numbers reflects exactly how seriously clinical communication is taken.
Exemptions from English testing are narrow. Generally, a nurse qualifies for an exemption only if their entire nursing education — not just the country, but the language of instruction and textbooks — was conducted in English in one of a specific list of recognized countries. That list includes the United Kingdom, Ireland, Australia, New Zealand, and Canada — but notably excludes Quebec, where clinical nursing education is conducted in French.
One practical risk worth flagging: standardized test scores expire. If you take an English exam early in your process and then experience delays — which is common in international nurse credentialing — you may need to retest before your VisaScreen certificate can be issued. Take the exam early, keep your score reports, and track the expiration dates.
Every nurse working as an RN in the United States must pass the NCLEX-RN, the national licensing examination. U.S.-trained nurses take it once upon graduation. For international nurses, it sits at the end of a credentialing sequence — you must clear the credential evaluation first, then the English exam, before most state boards will authorize you to sit for NCLEX.
The exam is not a knowledge test in the traditional sense. It is a clinical judgment test, built on a computer-adaptive platform that adjusts the difficulty of each question based on your previous answers. The current version — the Next Generation NCLEX — places particular emphasis on recognizing clinical cues, analyzing patient situations, and making evidence-based care decisions. Many internationally trained nurses find that their foundational nursing knowledge is strong but that the exam's approach to clinical reasoning requires specific preparation. Preparation time matters here.
One logistical point in your favor: the NCLEX is available at international testing centers in several countries, including India, the Philippines, the United Kingdom, Mexico, and Japan. You can pass the NCLEX before you ever apply for a visa. This is worth taking advantage of — completing the exam early locks in that credential and removes one item from the parallel checklist you will be managing during the immigration process.
One important distinction: passing the NCLEX does not grant you a license. It satisfies the examination requirement of the specific state board to which you applied. The board still needs to verify all your other documentation — credential evaluation, English scores, background check, identity verification — before issuing your license. And your choice of state board matters: processing timelines, documentation requirements, and eligibility for the Nurse Licensure Compact (which allows practice across multiple states) vary significantly. This is a decision worth thinking through carefully, ideally with input from an immigration attorney who understands how state licensure interacts with your overall immigration timeline.
This is the step that catches the most people off guard — because it exists at a level most nurses don't think to look.
Under Section 343 of the Illegal Immigration Reform and Immigrant Responsibility Act of 1996, any foreign healthcare worker seeking an occupational immigrant or nonimmigrant visa must obtain a federal screening certificate before their visa can be finalized. For nurses, that certificate is the VisaScreen, administered by CGFNS International.
U.S.-trained nurses working in the U.S. have no VisaScreen requirement. This is purely a federal immigration layer that applies to foreign workers in healthcare occupations.
The VisaScreen certificate confirms three things: that your foreign nursing education is equivalent to a U.S. nursing degree, that your professional licenses are valid, and that you meet English language proficiency standards. In other words, it synthesizes documentation from your nursing school, your home country licensing board, and your English testing agency — all verified at the primary source level.
That is exactly why it becomes a chokepoint. Each of those sources operates on its own timeline. A delay from your nursing school in sending transcripts, a lag in license verification from an overseas regulatory board, or a missing score report from a testing agency can each stall the entire certificate — even if every other piece is ready. One incomplete document holds everything.
The VisaScreen certificate is valid for five years. But "valid at filing" is not enough — it must still be valid at the time of your final green card interview. Nurses who started the process early, then experienced delays in the immigration queue, have arrived at their consular interview with a lapsed certificate and faced unexpected complications as a result.
The strategic lesson is simple: begin the VisaScreen process as early as possible — in parallel with your NCLEX preparation, not after. Do not treat it as a final step. Treat it as a parallel track that needs to be moving from day one.
State boards of nursing are not uniform. Each has its own additional requirements for foreign-educated applicants, and the variation matters.
Several states require applicants to provide a Social Security Number or Individual Taxpayer Identification Number (ITIN) before processing a license application. Maryland, for example, implemented this requirement in 2012. For nurses who have not yet entered the U.S. and do not have a Social Security Number, this creates a practical sequencing challenge. Some states have created workarounds — Maryland now allows ITIN holders to apply online — but navigating this correctly takes awareness of the specific rules in your target state.
Fingerprinting and state and federal criminal background checks are required in most states for foreign-educated applicants. Timing varies: electronic fingerprinting results typically return within a week; manual fingerprint cards can take three to four weeks. Some states will not issue an Authorization to Test for the NCLEX until background checks are cleared, so delays here cascade into everything downstream.
Some states also require international applicants to pass the CGFNS Qualifying Exam as a prerequisite to NCLEX eligibility. This is an additional examination designed to test foundational nursing knowledge before a candidate is admitted to the national exam. Not all states require it — but if yours does and you don't know about it, it will be a surprise at the worst possible time.
Finally, Nurse Licensure Compact eligibility — which allows an RN to practice in multiple member states on a single license — is affected by whether the nurse's SSN was on file at the time of initial application. Nurses who obtained a "Maryland Only" license without an SSN, for example, do not automatically gain NLC privileges until they update their records. If multi-state practice matters to you or your employer, this needs to be part of the plan from the beginning.
Most of the steps above happen before you arrive. This one happens after — and it is still required by most states before a foreign-educated nurse can practice independently.
The Foreign-Educated Nurse (FEN) course is a supervised clinical transition program, typically running approximately 240 hours, split evenly between classroom instruction and supervised clinical practice under a licensed U.S. RN. U.S.-trained nurses do not take this course. It exists specifically to bridge the gap between international nursing education and U.S. clinical practice.
The course covers areas that may not be immediately obvious to a nurse who is otherwise highly qualified: U.S. medical-legal standards and documentation requirements, the use of electronic health records (EHR) systems, U.S. medical equipment, and the specific communication expectations of American patients and families.
Clinical culture varies across countries in ways that experienced nurses sometimes underestimate. Standards for patient autonomy, family involvement in care decisions, documentation practices, and interprofessional communication in U.S. settings can feel genuinely different from what an internationally trained nurse is accustomed to — even one with years of strong experience. The FEN course, paired with a structured preceptor relationship in the first months, is where that gap closes.
Employers and recruitment agencies that invest in this transition support — dedicated clinical preceptors, thorough onboarding, cultural integration resources — tend to see significantly better long-term retention of international nurses. It is not just a regulatory box to check.
None of these credentialing steps happen in isolation. They run alongside the employer-driven immigration process — the prevailing wage determination, the I-140 petition filing, and the Visa Bulletin queue that determines when your green card can be finalized.
The VisaScreen certificate in particular must be in hand before your final green card interview, regardless of where your priority date stands in the queue. Nurses who let credentialing slip while focusing on the immigration timeline often find themselves ready on the government's schedule but not their own.
The practical implication is that these two tracks — credentialing and immigration — need to be mapped against a single timeline from the beginning, with attention to which steps can run in parallel and which are true prerequisites for what comes next. For a full explanation of the employer sponsorship process and how the Visa Bulletin affects your arrival date, see our article on EB-3 nurse sponsorship and Schedule A.
The additional requirements facing international nurses are not designed to be obstacles. They exist to ensure that every RN practicing in the United States — regardless of where they trained — meets the same standard of clinical competence and communication. That matters for patients.
What makes this process difficult is not any single step. It is the coordination: documents sourcing from institutions across multiple countries, deadlines in different agency systems, a credentialing track and an immigration track that must both stay on schedule simultaneously. A delay in one — a transcript that takes three months to arrive, an English score that expires, a VisaScreen document that lapses before the consular interview — affects everything else.
Whether you are an internationally trained nurse trying to map your own path to U.S. practice, or a healthcare employer trying to understand what your sponsored nurse needs to accomplish on their end, I can help you think through the sequencing and anticipate the friction points before they become delays.
Reach out to SG Legal Group to schedule a consultation. Consultations are available in English, Russian, and Romanian.
Disclaimer: The information provided in this article is for general informational purposes only and does not constitute legal advice. Immigration laws and policies are subject to change, and individual circumstances vary. For advice specific to your situation, please consult with a qualified immigration attorney.
Oleg Gherasimov, Esq.
Stay informed with our latest articles and resources.